https://threadreaderapp.com/thread/1280953660877529090.html
1/ This smart 2006 paper discusses the uselessness of lockdowns, masks, and school closings during epidemics.
More shocking: the lead authors are @T_Inglesby @JenniferNuzzo (two leading members of Team Apocalypse).
What's changed?
Not the science.https://t.co/y84Y2NkH5x
— Alex Berenson (@AlexBerenson) July 8, 2020
5/ On masks: "But studies have shown the ordinary surgical mask does little to prevent inhalation of small droplets bearing influenza virus. The pores in the mask become blocked by moisture from breathing, and the air stream simply diverts around the mask."
What's different now?
— Alex Berenson (@AlexBerenson) July 8, 2020
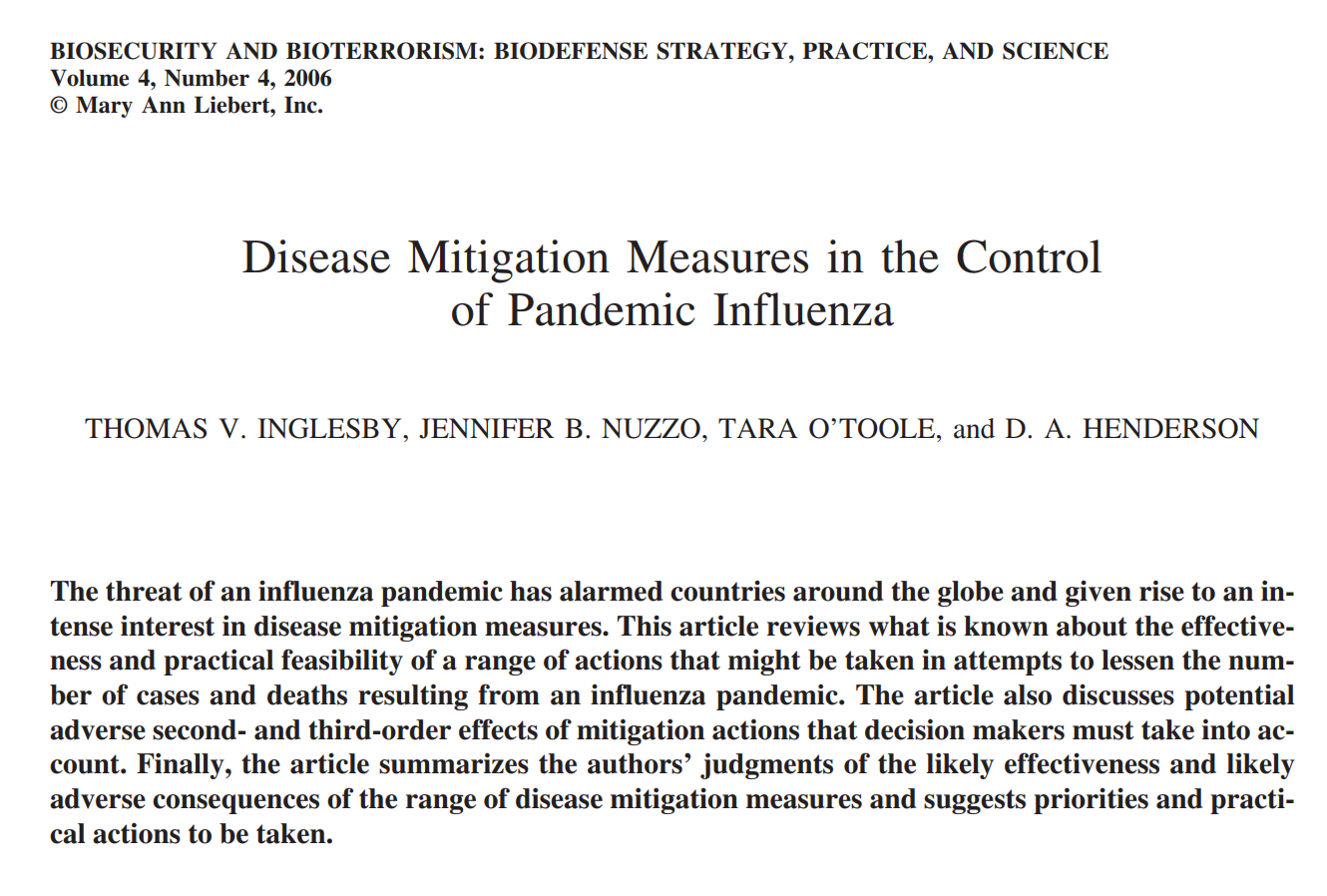
1/ This smart 2006 paper discusses the uselessness of lockdowns, masks, and school closings during epidemics.
More shocking: the lead authors are @T_Inglesby @JenniferNuzzo (two leading members of Team Apocalypse).
CEO and Director; and D. A. Henderson, MD, MPH, is Distinguished Scholar; all are at the Center for Biosecurity of the University of Pittsburgh Medical Center, Baltimore, Maryland.)What’s changed?Not the science.citeseerx.ist.psu.edu/viewdoc/downlo…
2/ The final paragraph begins:
“Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted.”
What’s changed, @T_Inglesby? What’s different now?
community disruption [are severe]…”What’s different now?
other likely points of assembly are closed (e.g., malls,
fast-food restaurants, churches, recreation centers, etc.)…”
4a/ “Such widespread closures, sustained throughout the pandemic, would almost certainly have serious adverse social and economic effects.”
What’s different now? What’s changed? (Aside from the fact that #SARSCoV2 is less dangerous/transmissible to children than the flu.)
5/ On masks: “But studies have shown the ordinary surgical mask does little to prevent inhalation of small droplets bearing influenza virus. The pores in the mask become blocked by moisture from breathing, and the air stream simply diverts around the mask.”
What’s different now?
6a/ “It is difficult to imagine how bus, rail, or air travelers could stay 3 feet apart from each other throughout an epidemic. And such a recommendation would greatly complicate normal daily tasks like grocery shopping, banking, and the like.”
What’s different now?
would have seriously disruptive consequences for a community…”
7b/ “But a policy calling for communitywide cancellation of public events seems inadvisable.”
What has changed, @T_Inglesby @JenniferNuzzo? Aside from the fact that #SARSCoV2 is so much LESS dangerous than the influenza strains that led you to make these recommendations?
8/ I mean, I know one thing has changed in 14 years.
But it’s not the science.
Please, help me out here. This is a serious question. Why shouldn’t we pay attention to you what you said THEN?
The WHO has stated that is no benefit to healthy people wearing masks in public, and there is only limited evidence that masks help when in contact with a sick person:
There is limited evidence that wearing a medical mask by healthy individuals in the households or among contacts of a sick patient, or among attendees of mass gatherings may be beneficial as a preventive measure. However, there is currently no evidence that wearing a mask (whether medical or other types) by healthy persons in the wider community setting, including universal community masking, can prevent them from infection with respiratory viruses, including COVID-19.
“Advice on the use of masks in the context of COVID-19”, WHO, April 6th 2020.
#
“both surgical and cotton masks seem to be ineffective in preventing the dissemination of SARS–CoV-2 from the coughs of patients with COVID-19 to the environment and external mask surface”
Experts from the Chicago School of Public Health do not recommend that the general public wear masks, for similar reasons to CIDRAP:
We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because: (1) There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission. (2) Their use may result in those wearing the masks to relax other distancing efforts because they have a sense of protection. (3) We need to preserve the supply of surgical masks for at-risk healthcare workers.
Brosseau L et al.. “Commentary: Masks-for-all for COVID-19 Not Based on Sound Data”, University of Illinois at Chicago School of Public Health, 2nd April 2020.
#
CDC’s Anthony Fauci admits to wearing a mask as a ‘symbol’ of what ‘you should be doing’ amid coronavirus
WASHINGTON – Top infectious disease specialist Dr. Anthony Fauci said Wednesday that he wears a mask as a “symbol” of what “you should be doing” during the coronavirus pandemic. “I want to protect myself and protect others, and also because I want to make it be a symbol for people to see that that’s the kind of thing you should be doing,” Fauci told CNN. When asked by host Jim Sciutto if his wearing of a mask encouraged their use, Fauci acknowledged masks aren’t “100% effective” but are a “valuable safeguard” and part of “respect for another person.” Fauci, director of the National Institute of Allergy and Infectious Diseases, said he walked around his Washington neighborhood and saw it was “very clear” that many people were wearing masks.
Video of Fauci saying mask are not necessary: https://twitter.
com/FuctupMike/status/ 1257868855986307072
Swiss Policy Research (SPR), founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics and receives no external funding.
‘Even in global ‘hotspots’, risk of death for general population of school & working age is in range of a daily car ride to work’
#
Update: Swiss Policy Research (SPR), founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics and receives no external funding.
On the effectiveness of masks
Various countries have introduced or are currently discussing the introduction of mandatory masks in public transport, in shopping malls, or generally in public.
Due to the lower-than-expected lethality of Covid-19 and the available treatment options, this discussion might become obsolete. The original argument regarding a reduction of hospitalizations (“flatten the curve”) is also no longer relevant, as the hospitalization rate was and is about twenty times lower than initially assumed.
Nevertheless, the question of the effectiveness of masks can be asked. In the case of influenza epidemics, the answer is already clear from a scientific point of view: masks in everyday life have no or very little effect. If used improperly, they can even increase the risk of infection.
Ironically, the best and most recent example of this is the often-mentioned Japan: Despite its ubiquitous masks, Japan experienced its most recent strong flu wave – with around five million people falling ill – just one year ago, in January and February 2019.
However, unlike SARS corona viruses, influenza viruses are transmitted also by children. Indeed, Japan had to close around ten thousand schools in 2019 due to acute outbreaks of the flu.
With the SARS 1 virus of 2002 and 2003, there is some evidence that medical masks can provide partial protection against infection. But SARS-1 spread almost exclusively in hospitals, i.e. in a professional environment, and hardly to the general public at large.
In contrast, a study from 2015 showed that the cloth masks in use today are permeable to 97% of viral particles due to their pore size and can further increase the risk of infection by storing moisture.
Some studies recently argued that everyday masks are nevertheless effective in the case of the new coronavirus and could at least prevent the infection of other people. However, these studies suffer from poor methodology and sometimes show the opposite of what they claim.
Typically, these studies ignore the effect of other simultaneous measures, the natural development of infection numbers, changes in test activity, or they compare countries with very different conditions.
An overview:
- A German study claimed that the introduction of compulsory masks in German cities had led to a decrease in infections. But the data does not support this: in some cities there was no change, in others a decrease, in others an increase in infections (see graph below). The city of Jena, presented as a model, simultaneously introduced the strictest quarantine rules in Germany, but the study did not mention this.
- A study in the journal PNAS claimed that masks had led to a decrease in infections in three hotspots (including New York City). This did not take into account the natural decrease in infections and other measures. The study was so flawed that over 40 scientists recommended that the study be withdrawn.
- A US study claimed that compulsory masks had led to a decrease in infections in 15 states. The study did not take into account that the incidence of infection was already declining in most states at that time. A comparison with other states was not made.
- A Canadian study claimed that countries with compulsory masks had fewer deaths than countries without compulsory masks. But the study compared African, Latin American, Asian and Eastern European countries with very different infection rates and population structures.
- A meta-study in the journal Lancet claimed that masks “could” lead to a reduction in the risk of infection, but the studies considered mainly hospitals (Sars-1) and the strength of the evidence was reported as “low”.
The medical benefit of compulsory masks therefore continues to remain questionable. In any case, a comparative study by the University of East Anglia came to the conclusion that compulsory masks had no measurable effect on the incidence of Covid infections or deaths.
It is also clear that widespread use of face masks couldn’t stop the initial outbreak in Wuhan.
Sweden showed that even without a lockdown, without compulsory masks and with one of the lowest intensive care bed capacities in Europe, hospitals need not be overburdened. In fact, Sweden’s annual all-cause mortality is in the range of previous flu seasons.
At any rate, authorities shouldn’t suggest to the population that compulsory masks reduce the risk of infection, for example in public transport, as there is no evidence of this. Whether with or without masks, there is an increased risk of infection in densely packed indoor areas.
Interestingly, the demand for a worldwide obligation to wear masks is led by a lobby group called “masks4all” (masks for all), which was founded by a “young leader” of the Davos forum.