A face covering signifies strength and compassion for others. Wearing one shows that you actually care about other people’s health.
— Governor Roy Cooper (@NC_Governor) May 26, 2020
ALERT: It's not about 'the science'! Fauci admits to wearing a mask as a 'symbol' of what 'you should be doing' amid coronavirus pandemic https://t.co/qEomSpRv1G via @usatoday
— Marc Morano (@ClimateDepot) May 28, 2020
WASHINGTON – Top infectious disease specialist Dr. Anthony Fauci said Wednesday that he wears a mask as a “symbol” of what “you should be doing” during the coronavirus pandemic. “I want to protect myself and protect others, and also because I want to make it be a symbol for people to see that that’s the kind of thing you should be doing,” Fauci told CNN. When asked by host Jim Sciutto if his wearing of a mask encouraged their use, Fauci acknowledged masks aren’t “100% effective” but are a “valuable safeguard” and part of “respect for another person.” Fauci, director of the National Institute of Allergy and Infectious Diseases, said he walked around his Washington neighborhood and saw it was “very clear” that many people were wearing masks.
#
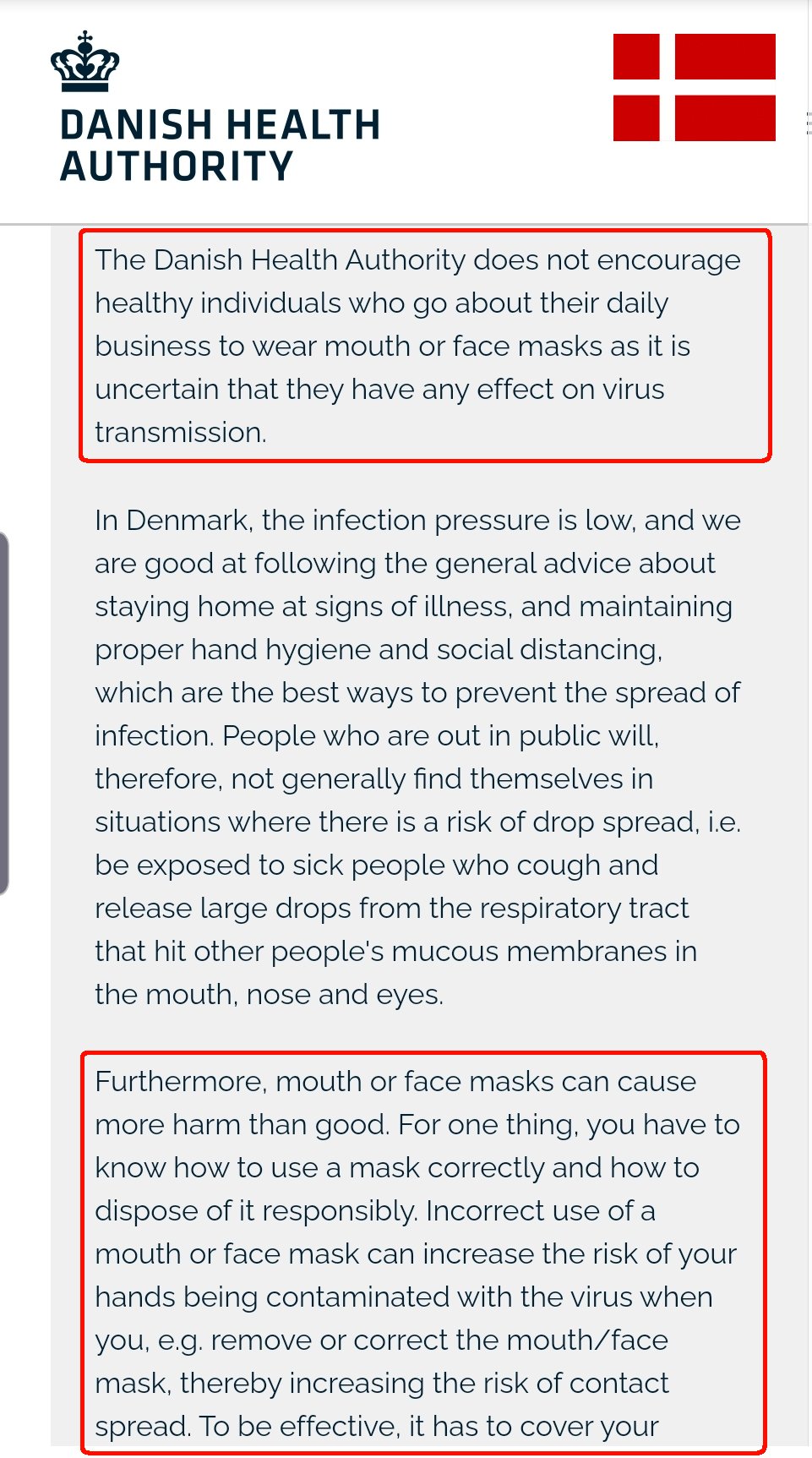
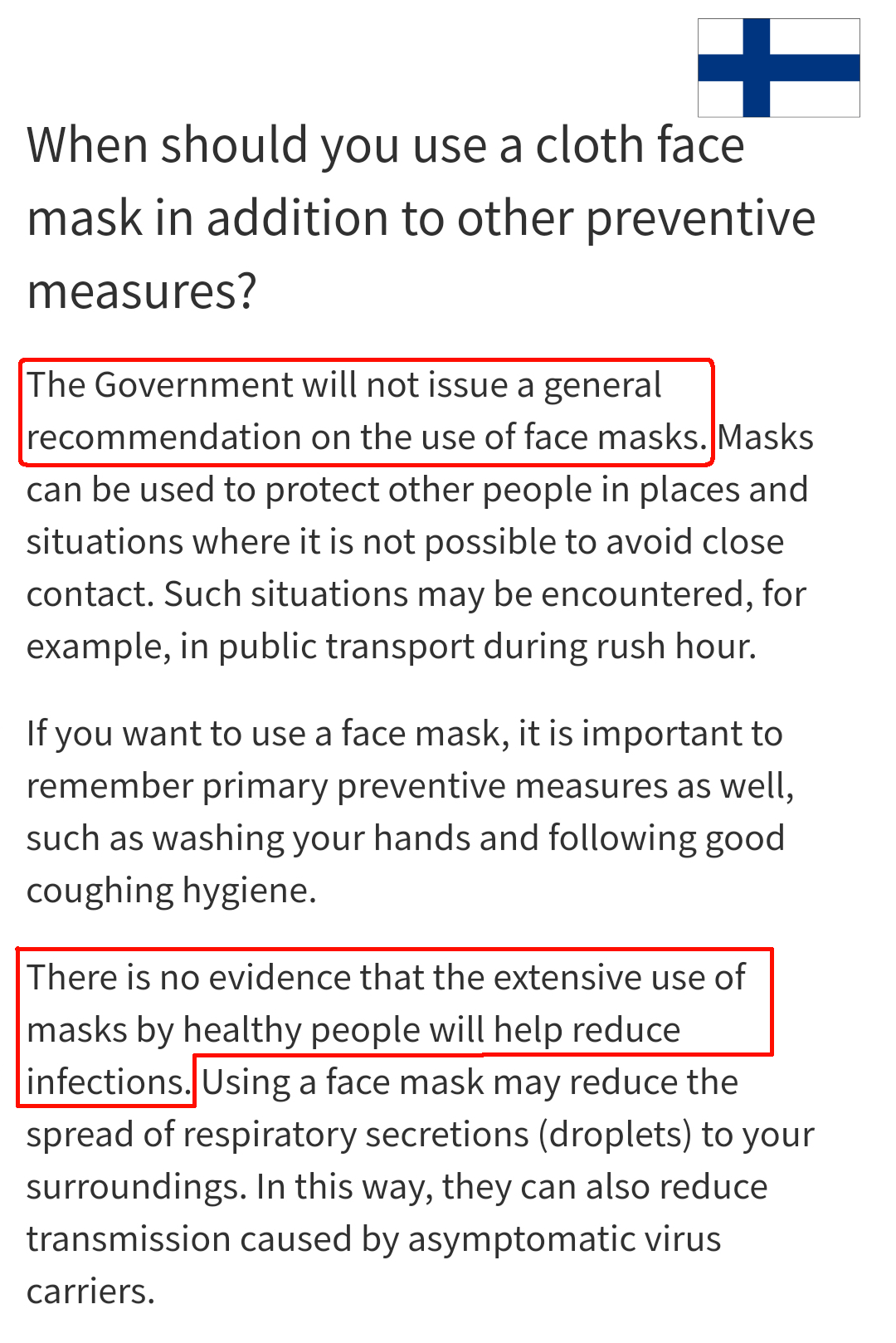
As we all know, Denmark, Finland, Norway, and Sweden are bigly red states, Trump supporters all the way. Otherwise why would their health authorities possibly question masks? https://t.co/7StdlAUGa3
— Alex Berenson (@AlexBerenson) June 25, 2020


Joe Biden: “I would do everything possible to make it required that people had to wear masks in public." https://t.co/t8YIuf2YLX
— Marc Morano (@ClimateDepot) June 26, 2020
#
Updated: Physicists mask study updated in August 2020
https://realclimatescience.com/2020/05/government-operating-in-a-science-vacuum/
Denis Rancourt is a PhD physicist, civil libertarian, and climate skeptic. He has interviewed me about climate for the Ontario Civil Liberties Association. Dr. Rancourt has an excellent paper out explaining why masks don’t work, and how governments are operating a science vacuum.
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy
By Denis G. Rancourt, PhD
Dr. Fauci also explained why people should not be wearing masks.
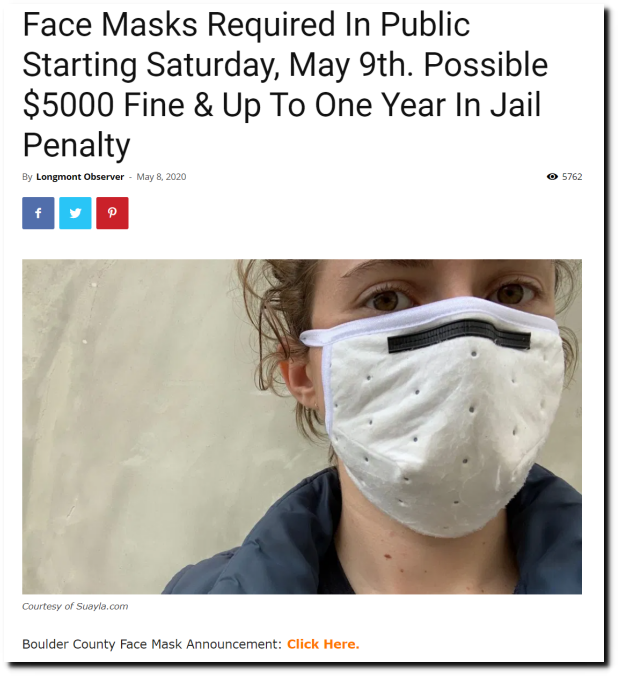
Yet in Boulder County, Colorado, you can get a year in jail for not wearing a mask. Just one more heinous abuse of science and human rights by Democrats.
I refuse to wear a mask, and make a point of smiling at everyone I see. I fled Boulder County to escape this nonsense, and now live in Cheyenne, Wyoming.
#
My interviews about the harms of masks and social distancing, with PERC, California. #MasksOff #COVID19 https://t.co/6gLdoHGCVY
— Denis Rancourt (@denisrancourt) May 20, 2020
This goes way beyond any virus. Fascism is a slow march and now it is in full bloom in liberal USA. https://t.co/90hXr3kdBx
— Denis Rancourt (@denisrancourt) May 10, 2020
#endthelockdown #COVIDー19 #thisisbullshit pic.twitter.com/rFzr0nGlOl
— Denis Rancourt (@denisrancourt) April 21, 2020
— Denis Rancourt (@denisrancourt) May 1, 2020
— Denis Rancourt (@denisrancourt) May 1, 2020
— Denis Rancourt (@denisrancourt) May 1, 2020
Follow the science! Fauci said mask unnecessary! Wsrh this clip of Fauci! Tweet from Marc Morano (@ClimateDepot)
Watch this! Fauci explains why wearing masks are a bad idea! (before the memo changed) Don't virtue signal! https://t.co/8x2FQKWbqA— Marc Morano (@ClimateDepot) May 9, 2020
https://twitter.com/MarkDog227/status/1259308578667667462
2/ Because here is an article PUBLISHED IN A @CDCgov journal (it’s dated May 2020 but was released Feb. 6) that reviews trials of masks (and handwashing) against influenza AND FINDS THEM USELESS. (More screenshots below.) https://t.co/JhgMsCv2e4 pic.twitter.com/K9kNdoT8Bf
— Alex Berenson (@AlexBerenson) May 12, 2020
"Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza."
— Marc Morano (@ClimateDepot) May 12, 2020
"There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure."
— Marc Morano (@ClimateDepot) May 12, 2020
According to the study: "We found no significant reduction in influenza transmission with the use of face masks."
— Marc Morano (@ClimateDepot) May 12, 2020
This study finds a Surgical mask does nearly nothing in stopping the SARS-Cov-2 Virus.
"both surgical and cotton masks seem to be ineffective in preventing the dissemination of SARS–CoV-2 from the coughs of patients with COVID-19 to the environment and external mask surface" pic.twitter.com/eVz8omguuj— JR4Truth (@JR4_Truth) May 12, 2020
Here's the original from CDC before they changed it to say that everyone should be wearing masks. pic.twitter.com/RQ1KO3uvpd
— Naturally Contrarian ✝️ (@Indiana_Patriot) May 28, 2020
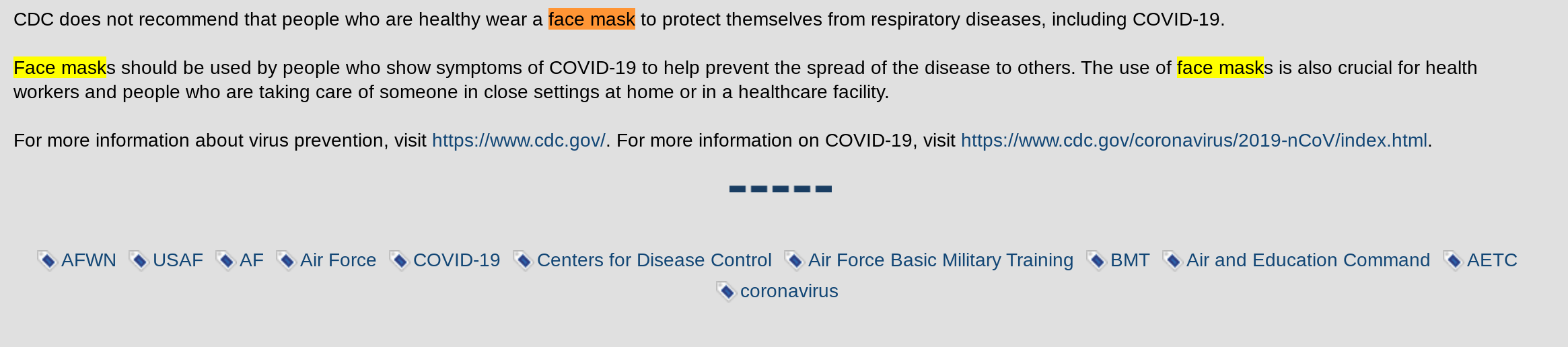
“CDC does not recommend that people who are healthy wear a face mask to protect themselves from respiratory diseases, including COVID-19.
Face masks should be used by people who show symptoms of COVID-19 to help prevent the spread of the disease to others. The use of face masks is also crucial for health workers and people who are taking care of someone in close settings at home or in a healthcare facility.”
For more information about virus prevention, visit https://www.cdc.gov/. For more information on COVID-19, visit https://www.cdc.gov/coronavirus/2019-nCoV/index.html.
On Memorial Day, we recall our war dead. A good time to remind everyone:
In March, governors and health officials took our freedom by exaggerating the risks of #SarsCov2.
Now they want to trade it back for masks and contact tracing and made-up rules.
No. Never.#teamreality
— Alex Berenson (@AlexBerenson) May 22, 2020
Got these masks '' anyone interested in buying one? pic.twitter.com/kMgKR6591U
— King Arthur & Excalibur (@OscarsWild1) May 20, 2020
Hey, remember these totally reasonable voluntary guidelines from a little place I call @cdcgov on March 16 – roughly 48 hours before we lost our minds? (I didn’t either.) pic.twitter.com/j0S9rArPTn
— Alex Berenson (@AlexBerenson) May 19, 2020
Actually, @ClimateDepot, I don't wear a mask because it's a sign of submission to tyrannical government.
Government officials are making these ridiculous mask dictates out of their own fear and CYA.
The "science" surrounding the effectiveness of masks is mixed at best. https://t.co/U0nxidkJOD
— Mark Mathis (@TheMarkMathis) May 14, 2020
Peak insanity: "Gov. Tom Wolf issued that Pa. residents should wear masks outside to protect those around you. This also applies to golfing, hiking and walking." https://t.co/7gplgA6evW via @lancasteronline
— Marc Morano (@ClimateDepot) June 18, 2020
— Marc Morano (@ClimateDepot) May 23, 2020
https://twitter.com/RememberPaoli/status/1264161434193350656
Gov Northam is a fan on vintage masks…
That's him on the right. pic.twitter.com/ct79mATSmW
— Andrew Follett (@AndrewCFollett) May 26, 2020
Thanks to the reader who pointed out this April 1 article touching on the uselessness of masks outside hospitals – it ran in a third-rate medical journal called @nejm – https://t.co/1ea5CegFfY pic.twitter.com/8EA4sgFeQP
— Alex Berenson (@AlexBerenson) May 28, 2020
Article in The New England Journal of Medicine April 2020: "We know that wearing a mask outside health care facilities offers little, if any, protection from infection."
— Marc Morano (@ClimateDepot) May 28, 2020
Article in The New England Journal of Medicine April 2020: "The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic."
— Marc Morano (@ClimateDepot) May 28, 2020
Experts are often called in, not to provide factual information or dispassionate analysis for the purpose of decision-making by responsible officials, but to give political cover for decisions already made and based on other considerations entirely.
— Thomas Sowell Quotes (@ThomasSowell) May 26, 2020
So this from @who is more or less definitive – masks are worthless for general use and for people who are asymptomatic/healthy. https://t.co/9vgEhk3Rxs
— Alex Berenson (@AlexBerenson) May 29, 2020
WHO Now Says Only Wear a Mask If You are Sick or Working with Sick — Otherwise You Don’t Need One
WHO: Coronavirus disease (COVID-19) advice for the public: When and how to use masks
Pandemic redux: 1918 vs. now, and the advent of “mask slackers” https://t.co/ztgtoDf2Vv
— Marc Morano (@ClimateDepot) May 29, 2020
1918: San Francisco required masks and had an anti-masking league form to resist mask wearing. People were arrested for not wearing masks and as we have seen today, violence sometimes resulted
— Marc Morano (@ClimateDepot) May 29, 2020
An “Anti-Mask” League formed there in staunch opposition to mask-wearing? Why? Businessmen said that even for open businesses the masks would hurt their sales because people supposedly didn’t want to venture out wearing masks
— Marc Morano (@ClimateDepot) May 29, 2020
Many people argued that they were ineffective (people wore gauze surgical masks made from cheesecloth) and that they were uncomfortable; and people protested that this was an unconscionable government interference with their freedom. Sounds familiar?
— Marc Morano (@ClimateDepot) May 29, 2020
1918 Anti-Mask Meeting pic.twitter.com/fv4c1NQwf5
— Marc Morano (@ClimateDepot) May 29, 2020
1918: 'Mask Slackers' arrested in San Francisco during Spanish Flu pic.twitter.com/roWsN1GQ5t
— Marc Morano (@ClimateDepot) May 29, 2020
1918: People shot over a 'mask slacker' pic.twitter.com/6puz5PRuEb
— Marc Morano (@ClimateDepot) May 29, 2020
Science supports no mandatory masks: Denis Rancourt, an eminent physics professor, former anarchist, and author, examined the scientific evidence for using face masks and respirators as preventative of contracting respiratory influenza-like disease, or respiratory illnesses believed to be transmitted by minuscule droplets. – “No RCT [randomized control trial] study with verified outcome shows a benefit for HCW [health care workers] or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions. The virions are super tiny, tinier than the pores in the respirators.” Rancourt writes, “if anything gets through (and it always does, irrespective of the mask), then you are going to be infected. Masks cannot possibly work. It is not surprising, therefore, that no bias-free study has ever found a benefit from wearing a mask or respirator in this application.”
Thomas Sowell: “Experts are often called in, not to provide factual information or dispassionate analysis for the purpose of decision-making by responsible officials, but to give political cover for decisions already made and based on other considerations entirely.”
Lockdowns failed to alter the course of pandemic and are now destroying millions of livelihoods worldwide, JP Morgan study claims – ‘Unlike rigorous testing of new drugs, lockdowns were administered with little consideration that they might not only cause economic devastation but potentially more deaths than Covid-19 itself,’ he claimed.
Prominent German Prof Says COVID-19 Lockdown “Completely Unnecessary”, “Unbelievably Damaging To The Economy” – “It is not the case that the reproduction number went down after the lockdown”, Professor Homburg says. “There are two points we can draw from this: First, the lockdown was not necessary because the number was below 1, and secondly, the lockdown was not effective because the number didn’t drop afterwards.”
We Didn’t Close America in 1957-1958 during ‘Asian flu’: Dealt with virus ‘without doing unacceptably massive damage to our whole society’ – “It ended up killing some 116,000 Americans—in a country that, with 170 million people, had about half the population of today’s America. Even using inflated numbers, about 95,000 have died so far from the coronavirus, by comparison…
But America in 1957 did not shut down. The National Football League played its games. Elvis Presley kept on wiggling his hips in concerts and TV shows (below, in a publicity still for that year’s “Jailhouse Rock”). The economy kept functioning, albeit with a greater number of people than usual calling in sick…
Americans were different in 1957-1958. Many had experienced two world wars, the Great Depression, and a Cold War that threatened to plunge the world into a nuclear holocaust. They understood that life inherently carries risks and that no government, however big, can shelter everyone from harm. Indeed, totalitarian governments in the 20th century had killed people by the tens of millions…
Unlike the coronavirus, it did not leave behind devastated small businesses, massive unemployment and a shattered economy. While the lockdowns are easing, some states today are still effectively making it a crime to run some businesses.”
'It’s like suffocating. Absolutely suffocating': Hot Temperatures Complicate Coronavirus Face Mask Safetyhttps://t.co/rTcM4CN5w8
— Marc Morano (@ClimateDepot) June 10, 2020
“The heat and humidity build up in your mask and make a beautiful breeding ground for bacteria,” he said.
— Marc Morano (@ClimateDepot) June 10, 2020
WHO now backs masks as COVID precaution: WHO says 'anecdotal evidence' of the benefits of wearing masks in crowds has prompted it to change position.
Or: Politics has forced it o change position. The 'science' must be in line with desired mask mandates. https://t.co/faxIZR20fL— Marc Morano (@ClimateDepot) June 6, 2020
Scientific Information on Masks Against COVID-19
5 June 2020by David Crowe
Masks are being widely recommended as protection against the COVID-19 virus, both to protect the wearer from infection and to protect others from those who do not know that they are infected. The trouble is that most of the scientific evidence and recommendations are against the use of masks by the general public, and some harms from wearing masks have been documented. Despite this, they are increasingly mandated. In some places you can’t walk around outside without a mask, and in others you can’t go inside a public space without a mask. Workers are often mandated to wear them – and now airline passengers, no matter the length of their flight.
Evidence for the use of masks
The strongest evidence for the use of masks is a Cochrane Collaboration review entitled “Physical interventions to interrupt or reduce the spread of respiratory viruses”. Seven studies were included in this review from the era of SARS. All of the studies that found mask wearing to be effective were case-control studies: a type of study that is subject to bias because the control arm is simply a representative group, with each “case” matched to a “control” by characteristics like age and sex, unlike in a placebo-controlled trial (which would admittedly be very difficult with masks). If the controls differ from the cases in characteristics that are not part of the matching – such as health or socio-economic status – differences may be found due to these uncontrolled variables, including in whether they chose to wear a mask.
Of the seven papers, five studied only healthcare workers, and I do not question whether healthcare workers should wear masks. This leaves only two papers concerning mask wearing by the general public. One provided no socio-economic or health data on the case-versus-control groups, leaving open the possibility that there were differences. The second study confirmed that the cases (who had been diagnosed with “probable” SARS; i.e., with symptoms and contact with another SARS victim, but without a SARS test) were significantly sicker than the controls. This makes sense because people who were diagnosed with SARS tended to have pre-existing health conditions, just as is found with COVID-19. Mask-wearing and hand-washing were more common in controls, resulting in the conclusion that they were protective. Attending farmers’ markets was also “protective” – but in reality probably just reflects the better health and therefore mobility of the control group. Really sick people may avoid the use of masks because it interferes with their breathing when they already have health problems or simply because they go out less. This possibility was not considered by either paper.
So, in conclusion, there are two papers that claim that wearing masks was protective against SARS, but one admits that the control group was significantly healthier than the case group, and the other paper is silent on this important source of bias.
There are also the hamsters, however. No, Hong Kong University did not find a source of hamster-sized surgical masks, but in an unpublished paper they describe putting a surgical mask over the air flow between a cage of RNA positive hamsters and a cage of RNA negative hamsters, and documenting that a higher proportion of the RNA-negative hamsters became RNA-positive when there was no mask over the airflow. It is not clear why the researchers believe their studies can be extrapolated directly to people. Although newspaper articles claim that the paper has been “released”, not even the Hong Kong University press release – the institution where the work was performed – provided any details about its location.
Evidence against the use of masks
A very recent review of the literature that was published in the CDC journal Emerging Infectious Diseases did not find evidence that masks (or hand-washing) were protective against influenza. Masks did not help infected people reduce their risk of infecting others, nor reduce the risk of uninfected people contracting influenza:
In this review, we did not find evidence to support a protective effect of personal protective measures or environmental measures in reducing influenza transmission. […] Hand hygiene is a widely used intervention and has been shown to effectively reduce the transmission of gastrointestinal infections and respiratory infections. However, in our systematic review, updating the findings of Wong et al., we did not find evidence of a major effect of hand hygiene on laboratory-confirmed influenza virus transmission. […] We did not find evidence that surgical-type face masks are effective in reducing laboratory-confirmed influenza transmission, either when worn by infected persons (source control) or by persons in the general community to reduce their susceptibility. […] It is essential to note that the mechanisms of person-to-person transmission in the community have not been fully determined. Controversy remains over the role of transmission through fine-particle aerosols.
Xiao J et al., “Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings – Personal Protective and Environmental Measures”, Emerg Infect Dis., May 17th 2020; 26(5).
A Korean study put masks on COVID-19 infected people and did not reduce the transmission of droplets when patients coughed with a mask on:
Neither surgical nor cotton masks effectively filtered SARS–CoV-2 during coughs by infected patients.
Bae S et al., “Effectiveness of Surgical and Cotton Masks in Blocking SARS-CoV-2: A Controlled Comparison in 4 Patients”, Ann Intern Med., April 6th 2020.
Adverse consequences of masks
Adverse consequences of masks are most obvious among healthcare workers, where use is more controlled; but members of the general public who voluntarily wear masks for extended periods of time may experience similar problems.
A study in the BMJ showed that people who were told to wear cloth masks for extended periods of time (for the purposes of the study) had higher rates of influenza-like illness (“ILI”) than other healthcare workers who could decide if and when to wear masks, and had higher rates of ILI than those wearing surgical masks:
The rates of all infection outcomes were highest in the cloth mask arm, with the rate of ILI statistically significantly higher in the cloth mask arm [13 times higher] compared with the medical mask arm. Cloth masks also had significantly higher rates of ILI compared with the control arm [workers who followed standard practice, which could sometimes include mask wearing]. An analysis by mask use showed ILI and laboratory-confirmed virus were significantly higher [6.64 times for ILI and 1.72 times higher for lab confirmed virus] in the cloth masks group compared with the medical masks group. Penetration of cloth masks by particles was almost 97% and medical masks 44%.”
MacIntyre CR et al., “A cluster randomised trial of cloth masks compared with medical masks in healthcare workers”, BMJ Open, April 22nd 2015; 5(4): e006577.
A study from Singapore found an increased risk of headaches – indicative of oxygen deprivation – among healthcare workers. This may or may not apply to the general public, who generally wear masks that are less tight-fitting (and therefore less effective):
A total of 158 healthcare workers participated in the study. Majority [126/158 (77.8%)] were aged 21–35 years. Participants included nurses [102/158 (64.6%)], doctors [51/158 (32.3%)], and paramedical staff [5/158 (3.2%)]. Pre-existing primary headache diagnosis was present in about a third [46/158 (29.1%)] of respondents. Those based at the emergency department had higher average daily duration of combined PPE exposure compared to those working in isolation wards [7.0 vs 5.2 hours] or medical ICU [7.0 vs 2.2 hours]. Out of 158 respondents, 128 (81.0%) respondents developed de novo PPE-associated headaches. A pre-existing primary headache diagnosis (OR = 4.20 and combined PPE usage for >4 hours per day (OR 3.91) were independently associated with de novo PPE-associated headaches. Since COVID-19 outbreak, 42/46 (91.3%) of respondents with pre-existing headache diagnosis either “agreed” or “strongly agreed” that the increased PPE usage had affected the control of their background headaches, which affected their level of work performance.
Ong JJY et al., “Headaches Associated With Personal Protective Equipment – A Cross-Sectional Study Among Frontline Healthcare Workers During COVID‐19”, Headache, May 2020; 60(5): 864-877.
Opinions against the use of masks
The WHO has stated that is no benefit to healthy people wearing masks in public, and there is only limited evidence that masks help when in contact with a sick person:
There is limited evidence that wearing a medical mask by healthy individuals in the households or among contacts of a sick patient, or among attendees of mass gatherings may be beneficial as a preventive measure. However, there is currently no evidence that wearing a mask (whether medical or other types) by healthy persons in the wider community setting, including universal community masking, can prevent them from infection with respiratory viruses, including COVID-19.
“Advice on the use of masks in the context of COVID-19”, WHO, April 6th 2020.
The University of Minnesota Center for Infectious Disease Research and Policy (CIDRAP) does not recommend that the public wears masks, because they do not work, they may reduce other preventive measures, and they risk the supply of masks for healthcare workers:
We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because: There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission Their use may result in those wearing the masks to relax other distancing efforts because they have a sense of protection. We need to preserve the supply of surgical masks for at-risk healthcare workers.
Brosseau LM et al., “COMMENTARY: Masks-for-all for COVID-19 not based on sound data”, CIDRAP, April 1st 2020.
Experts from the Chicago School of Public Health do not recommend that the general public wear masks, for similar reasons to CIDRAP:
We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because: (1) There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission. (2) Their use may result in those wearing the masks to relax other distancing efforts because they have a sense of protection. (3) We need to preserve the supply of surgical masks for at-risk healthcare workers.
Brosseau L et al.. “Commentary: Masks-for-all for COVID-19 Not Based on Sound Data”, University of Illinois at Chicago School of Public Health, 2nd April 2020.
An experienced ER nurse (RN, MSN) examined the data when her grandchild’s pre-school decided that even toddlers need to wear masks, and her literature review produced a lot of information against mask wearing, and she showed that the seven papers by the CDC in support of mask wearing are irrelevant to the subject.
Conclusions
Evidence is largely against mask-wearing by the general public. It is generally seen as ineffective, may take attention away from other protective measures, will reduce the supply of masks for healthcare workers and may cause harm when worn for extended periods of time.
#
Fauci says claiming masks don't work initially was a "noble lie." https://t.co/edDV55Ym7v
— Gerard Pinzone (@GerardPinzone) June 19, 2020
Fauci now says that they told us masks are unnecessary because there was a shortage. Ok…..except now any mask will do. They could have said from day 1 that any cloth mask would do. They did not.
— Startingover (@JerseygirlSusan) June 19, 2020
Here’s why we mandate masks… pic.twitter.com/q0KohLfFAr
— Jon Tigges (@jontigges) June 19, 2020
https://twitter.com/DrEdwinLau/status/1273829843604398080
WHOs latest mask recommendations including the following benefits of masks. Making people "feel" like they play a role. pic.twitter.com/lLUJpcGwiI
— JR4Truth (@JR4_Truth) June 19, 2020
This isn't a ringing endorsement. From the article:
1) "Surgical masks". Not what 90+% are wearing.
2) "Could"
3) "from symptomatic"
That summarization doesn't support the need for healthy individuals to tie an old cut up t-shirt around their face. pic.twitter.com/2XSqgfzQBA
— Matt Ward (@Tchu819) June 19, 2020
The Coronavirus Mask Charade Continues
1/ This is quite the paper on masks, published in @BMJ_Open in 2015: a randomized trial (the gold standard, yadda yadda) of 1600 health-care workers showed those wearing masks were 6 times (!) as likely to have flu-like illnesses as those in the control group after 4 weeks… pic.twitter.com/pst5aw9b0C
— Alex Berenson (@AlexBerenson) July 8, 2020
2/ The conclusion: “This study is the first RCT of cloth masks, and the results caution against the use of cloth masks… moisture retention, reuse of cloth masks, and poor filtration may result in an increased risk of infection.” https://t.co/iSBvpWPh8I
— Alex Berenson (@AlexBerenson) July 8, 2020
3/ My mask protects you! By getting me too sick to go outside… https://t.co/iSBvpWPh8I
— Alex Berenson (@AlexBerenson) July 8, 2020